-
Address:
17888 67th Court North
Loxahatchee, FL
-
Mail us:
contact@wrightacademia.org
- submit manuscript
Case Report |
Open Access |
Volume 1 | Issue 1 |
Terlipressin Induced Cardiac Arrest: A Case Report
Mads J Niemann and Abbas A Qayyum
Department of Cardiology, Hvidovre Hospital, Denmark
*Corresponding author: Mads Jacob Niemann, MD, Department of Cardiology, Hvidovre Hospital, Kettegaard Alle 30, DK-2650 Hvidovre, Denmark, Tel: +4560633752, E-mail: mads.jacob.niemann@regionh.dk
Citation: Niemann MJ, Qayyum AA (2019) Terlipressin Induced Cardiac Arrest: A Case Report. Cardiol Cases Syst Rev. 1:001.
Copyright © Niemann MJ, et al.
Received: |
Accepted: |
Published: |
Terlipressin is a vasoconstrictor with effect on vascular smooth muscles in the portal and splanchnic circulation, thereby decreasing blood pressure in esophagus varices. Therefore, terlipressin is recommended as first-line of pharmacological therapy in patients with bleeding esophagus varices. Terlipressin has been reported in a few cases to induce prolonged QT interval causing cardiac arrhythmias, mostly Torsade de Pointes. In this case report, a 34-year-old woman admitted with upper gastrointestinal bleeding were treated with terlipressin and subsequently had cardiac arrest. Monitoring during cardiac arrest showed ventricular fibrillation. After return of circulation, laboratory results showed hypokalemia and hypomagnesemia. Other likely causes to cardiac arrest were ruled out by clinical examination, chest x-ray and echocardiography. ECG showed prolonged QT interval. The administration of terlipressin, the hypokalemia and the hypomagnesemia may all be either cause or a contribution to ventricular fibrillation. In conclusion, this case report illustrates the importance of measurement of electrolytes upon admission along with observation of the patient during and after administration of terlipressin.
Introduction
Increased portal venous pressure causes esophagus varices, mostly due to liver cirrhosis. Esophagus varices have a potential risk of bleeding and an acute esophageal bleeding is associated with a 20-50% mortality [1]. The guideline of World Gastroenterology Organization for treatment of bleeding esophagus varices has terlipressin-infusion as first-line of pharmacological therapy followed by gastroscopic banding of the bleeding site during the first 12 hours of hospitalization [2]. Terlipressin has been showed to reduce mortality, rebleeding and failure of hemostasis [3]. However, only a few case reports have been published about the serious side effect of terlipressin infusion resulting in cardiac arrhythmia (Table 1).
Terlipressin
The prodrug terlipressin used to treat esophagus varices is cleaved enzymatic to lysinvasopressin, a synthetic antidiuretic hormone. Approximately, 30 min after intravenous injection of terlipressin, lysinvasopressin can be detected in plasma and maximum concentration occurs after 1-2 hours. Terlipressin has a plasma half-life of 40 min and is 99% metabolized by peptidases. The effect of terlipressin is primarily vasoconstrictive on vascular smooth muscles in the portal and splanchnic circulation, which is mediated by V1a receptors. This causes a decrease in esophageal venous blood pressure and thus the clinically required effect - hemostasis. However, terlipressin can increase systemic mean arterial pressure, which is also mediated by V1a receptors. The increased pressure can trigger a decrease in heart rate mediated by glomus caroticum. This bradycardic effect can further be amplified by all drugs known to cause bradycardia [4-8].
Case Presentation
A 34-years-old unmedicated female known with anorexia, chronic alcoholism, liver cirrhosis and esophagus varices grade 1-2 was admitted to the emergency department due to upper gastrointestinal bleeding. Initially 2 mg terlipressin was administrated intravenously every 4 hours. Terlipressin infusion had no hemodynamic effect on the patient. On the second day gastroscopy confirmed bleeding esophagus varix, which was banded. After 36 hours of hemostasis, terlipressin was reduced to 1 mg every 4 hours. On the third day of hospitalization, the patient was found with unwitnessed cardiac arrest. 30 min previously, she had received 1 mg of terlipressin intravenously. Cardiopulmonary resuscitation according to European resuscitation guidelines was immediately started. Initial rhythm was ventricular fibrillation. All seven assessments of rhythm showed ventricular fibrillation. Return of spontaneous circulation (ROSC) occurred after 25 min of resuscitation. Bedside transthoracic echocardiography showed left ventricle ejection fraction on 50%, general myocardial hypokinesia but no sign of cardiac tamponade or dilated right ventricle. ECG post-ROSC showed global ST-depressions (Figure 1A) but normalized quickly in serial ECG taken 15 min and 25 hours after ROSC (Figure 1B and Figure 1C). Prolonged QT interval (QTc 580 ms) was seen 25 hours after ROSC (Figure 1C). Troponin I was measured to 170 ng/L (reference 24 ng/L) 2 hours after ROSC, reached a maximum on 515 ng/L, 7 hours after ROSC and decreased afterwards. Clinically, there was no suspicion of an acute myocardial infarction, and ECG and troponin changes were considered related to cardiopulmonary resuscitation. Chest x-ray was without any pathology. Terlipressin was discontinued.
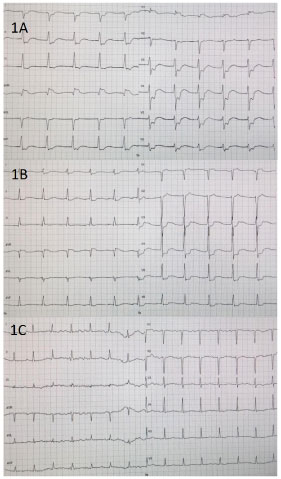
Figure 1: (a) ECG taken 3 min; (b) 15 min; (C) 25 hourspost-ROSC.
At the time of admission, the patient was slightly hypokalemic with a potassium on 3.3 mmol/L (reference 3.5-4.6 mmol/L). Supplements were administered. On the day of cardiac arrest, potassium had decreased to 2.1 mmol/L. Post-ROSC, the patient had hypomagnesemia on 0.64 mmol/L (reference 0.70-1.10 mmol/L) and supplements were given. Terlipressin was discontinued. The patient was transferred to intensive care unit without any new arrhythmias but died two weeks later due to hepatic encephalopathy.
Discussion
Terlipressin is known to induce QT prolongation. This may be enhanced by electrolyte abnormalities and by medication known to prolong QT interval. This case report illustrates the importance of measurement of electrolytes at the time of admission along with observation of patient during and after administration of terlipressin. The administration of terlipressin, the hypokalemia and hypomagnesemia might all be either cause or a contributor to ventricular fibrillation. In high-risk patients, cardiac monitoring should be considered.
Conflicts of Interest
None declared.
Source of Funding
None declared.
References
- Ioannou GN, Doust J, Rockey DC (2003) Systematic review: Terlipressin in acute oesophageal variceal haemorrhage. Aliment Pharmacol Ther 17: 53-64.
- LaBrecque D, Khan AG, Sarin SK, Mair AW Le (2014) World Gastroenterology Organisation Global Guidlines: Esophageal Varices.
- Krag A, Borup T, Møller S, Bendtsen F (2008) Efficacy and Safety of Terlipressin in Cirrhotic Patients with Variceal Bleeding or Hepatorenal Syndrome Advances in Therapy ®. Adv Ther 25: 1105-1140.
- Anon. GLYPRESSIN ® Solution for Injection.
- Jao YTFN (2016) Refractory torsade de pointes induced by terlipressin (Glypressin). Int J Cardiol 222:135-140.
- Garg Y, Kumar SB, Paul RA, Jindal S (2016) Terlipressin Induced Ventricular Tachycardia. Chettinad Heal City Med J 5: 94-95.
- Lehmann M, Bruns T, Herrmann A, Fritzenwanger M, Stallmach A (2010) 54-year-old man with cirrhosis and therapy-related torsades de pointes tachycardias. Internist Online 52: 445-450.
- Ürge J, Sincl F, Procházka V, Urbánek K (2008) Terlipressin-induced ventricular arrhythmia. Scand J Gastroentero l43: 1145-1148.
Table 1: Cases of terlipressin-induced arrhythmias. View Table 1