-
Address:
17888 67th Court North
Loxahatchee, FL
-
Mail us:
contact@wrightacademia.org
- submit manuscript
Review Article |
Open Access |
Volume 2 | Issue 1 |
Diagnostic and Therapeutical Pathway in a Patient Presenting with Simultaneous Neurological and Cardiac Symptoms
Katharina Birkl, Gudrun Feuchtner, Fabian Plank, Christoph Beyer, and Guy J Friedrich
Cardiology and Radiology Departments, Medical University Innsbruck, Austria
*Corresponding author: Guy J. Friedrich, MD, Universitatsklink Innere Medizin III, Kardiologie Anichstrasse 35, A-6020 Innsbruck, Austria; Tel: +43 512 504 81113; Fax: +43 512 504 22767; E-mail: guy.friedrich@tirol-kliniken.at
Citation: Birkl K, Feuchtner G, Plank F, Beyer C, Friedrich GJ (2020) Diagnostic and Therapeutical Pathway in a Patient Presenting with Simultaneous Neurological and Cardiac Symptoms. Cardiol Cases Syst Rev. 2:007.
Copyright © Birkl K, et al.
Received: |
Accepted: |
Published: |
We report a 80 year old female patient with ambivalent neurological and cardiac symptoms. Due to guideline conform diagnostic pathways a fast diagnosis of either cerebro - or cardiovascular pathology is mandatory to prevent potential ischemic damage.
Cooperation of several multidisciplinary teams with high imaging as well as vascular medical experience may lead to the right diagnosis and reveal unexpected pathologies. This approach may avoid unnecessary invasive procedures causing therapeutical delays. Moreover individually tailored medical therapy may be started immediately and lead to complete recovery of the patient's disease.
Introduction
In patients presenting at the emergency room with ambivalent vascular symptoms of unclear origin it may be difficult to get a fast and precise diagnosis. However, this may be crucial to reach successful therapy in the setting of a life threatening scenario.
Multidisciplinary cooperation between radiologists, neurovascular and cardiovascular specialists may be the clue for a non-delayed good clinical outcome in these patients.
Clinical Report
A 80 year old female patient is presenting at the internal medicine emergency department with atypical chest pain and numbness on her left hand. After a transient, more severe chest pain event one week before without medical contact (due to the start of a short vacation), the patient was seen by her general practice physician after her return. After a positive troponin T rapid assay and the symptoms described above he sent the patient to the emergency service.
Former clinical history of the patient included a transient ischemic attack (TIA) of the right artery cerebral media in December 2017 without remaining pathology. Premedication since then was 100 mg aspirin once a day.
ECG revealed slow R-wave progression in V1-V4 with ST elevation (Figure 1). CK values were normal and troponin T elevated (150 ng/l).
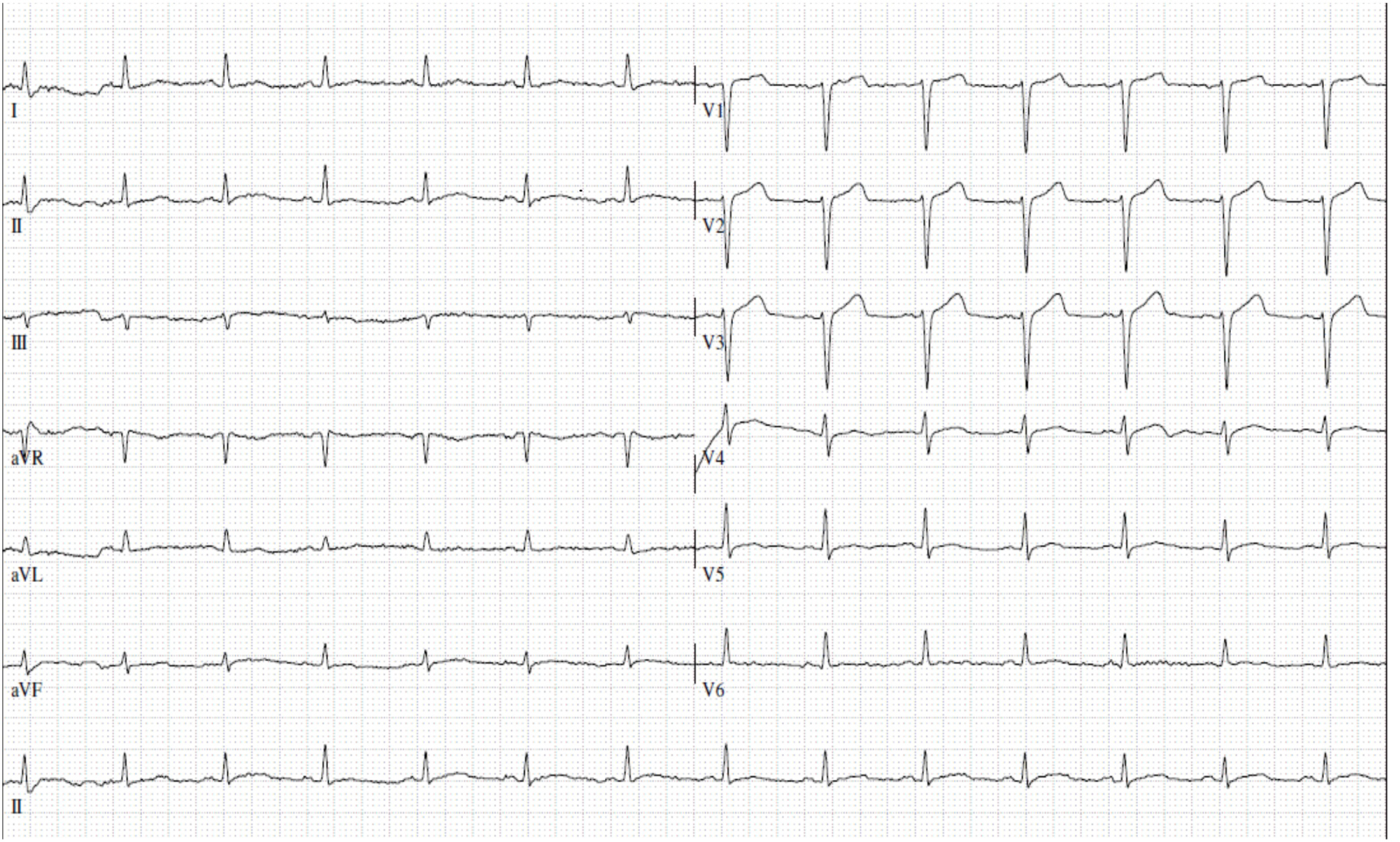
Figure 1: EKG ad admission.
All other blood sample values were in the standard range. Symptom based neurological examination was performed and a pure sensoric TIA, probably related to a cardioembolic origin, diagnosed. The following cerebral CT revealed no acute infarction areas.
Based on chest pain history and actual clinical presentation we performed triple rule out thoracic CT in search for possible coronary, aortic or pulmonary embolic disease. The latter were both excluded, but coronary CT revealed diffuse atherosclerosis without evidence of significant stenoses.
Due to this report and disappearance of chest pain symptoms we did not opt for immediate invasive coronary angiography. Furthermore CT angiography revealed several larger left ventricular thrombi (LVT) mostly located in the apical segment. (Figure 2).
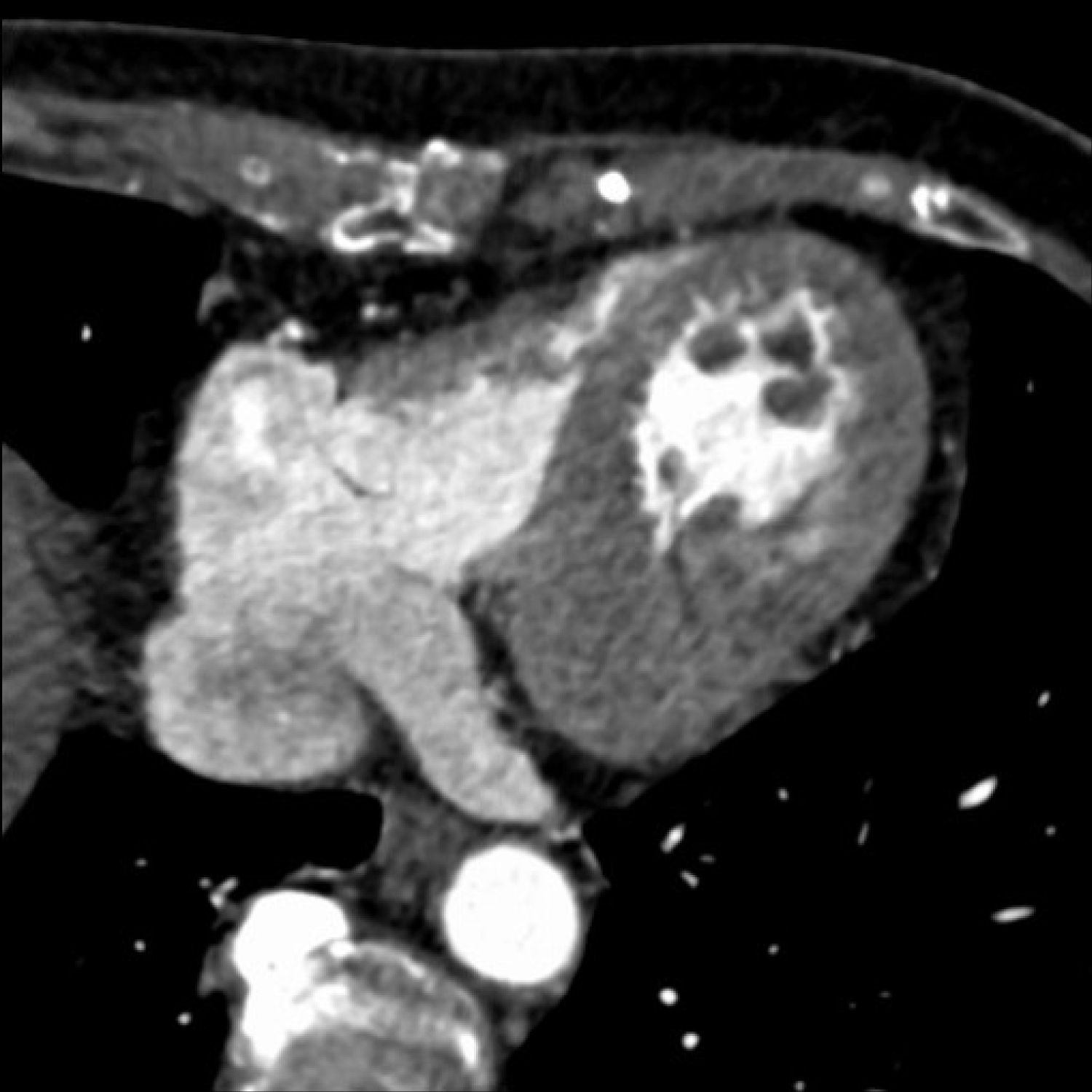
Figure 2: CT angiography with presence of larger left ventricular thrombi.
Transthoracic echocardiography confirmed at least three mobile thrombotic masses in the left ventricle with apical hypokinesia and minor globally reduced left ventricular ejection fraction of 45%.
Initial intravenous heparin perfusion was started for several days. On the seventh day an elective invasive coronary angiography was performed and a 30% stenosis of the proximal LAD and diffuse sclerotic disease in CX and RCA were found (Figure 3).
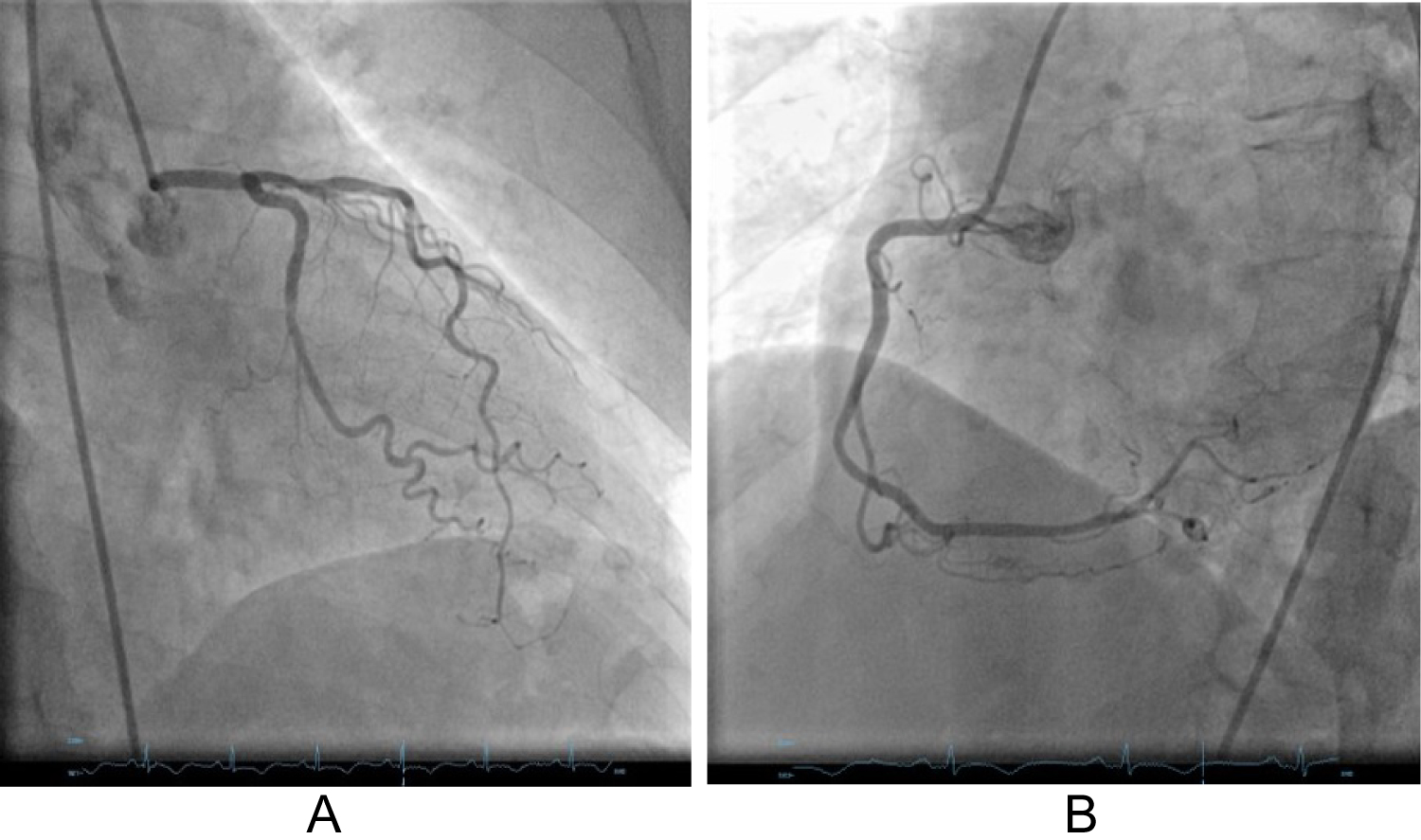
Figure 3A and 3B: Invasive coronary angiography of left and right coronary arteries showing diffuse coronary sclerosis without significant stenosis.
The patient was now classified as a delayed acute coronary syndrome (ACS) case with self healing and spontaneous recanalization of the proximal LAD a week before presentation at our emergency department. The subsequent myocardial infarction was clinically well tolerated by the patient but, due to hypo- akinetic regional wall dysfunction, apical thrombi developed and caused neurologic embolic symptoms. This was fostered by the absence of immediately available adequate medical therapy.
After one week of unfractionated heparin, medication was switched to triple therapy with aspirin 100 mg , clopidogrel 75 mg daily and edoxaban 30 mg daily for another 4 weeks, then reduced to edoxaban 30 mg and clopidogrel 75 mg daily.
Transthoracic echo after 3 months revealed a normal left ventricular function with no more thrombi detectable. In the mean time the patient was angina free and had no signs of embolic neurology symptoms.
The final medication of the patient resulted in 100 mg aspirin a day beside beta blocker, statin and ACE inhibition.
Discussion
The clinical presentation of the patient was ambiguous because of unclear origin. Numbness in the arm and atypical chest pain may represent a symptom related to cardiac ischemia as well as additional cerebrovascular disease. The complexity of the current case resulted from the paramount question of how to react first in the setting of a potentially lifethreatening vascular problem with need for immediate therapy. The differentiation between an acute neurological and/or cardiac problem and a potential call for rapid action to avoid a more prominent ischemic or embolic myocardial or cerebral damage was intriguing.
Symptoms of the patient were requiring coordination of multiple medical specialities: a probable cardiologic diagnosis could have ranged from a Tako tsubo cardiomyopathy to an acute coronary syndrome, the neurological symptoms could have been related to primary or secondary acute cerebrovascular pathology with need for immediate therapy.
Clinical presentation of the patient led us consider 2 major differential diagnoses: delayed myocardial infarction with persisting symptoms and Takotsubo cardiomyopathy with possible embolic coronary and cerebral embolism. Following the international Takotsubo diagnostic criteria [1] some were fulfilled except 2 common findings: no apical ballooning and no emotional, physical or combined trigger preceeding the event.
The stable hemodynamic conditions of the patient allowed us to perform a non- invasive imaging diagnostic pathway including triple rule out thoracic CT for detection of CAD, aortic and pulmonary disease as well as cerebral CT and echocardiography. Triple rule out computer tomography has been described to be an imaging modality with high predictive performance in patients with acute chest pain [2]. Moreover it has been recently shown that CT angiography may be a promising alternative for detection of cardiac thrombi compared to echocardiography [3].
Left ventricular thrombi after myocardial infarction (mostly located on the anterior wall) are a more frequent finding than formerly expected and may lead to embolic complications and are associated with a very high risk of MACE [4,5].
These findings are considerably changing the post MI medical strategy requiring a different antiplatelet and anticoagulative therapy. Standard antithrombotic therapy in patients with cardiac intracaval thrombi is heparin perfusion and subsequent OAC medication with warfarin or coumarin [6].
In selected cases however, when in combination with an antiplatelet medication and underlying coronary artery disease, a less aggressive approach should be applied to the high risk of occurring bleeding events.
Even in the absence of randomized studies using DOACs in these indications, publications in patients with need for oral anticoagulation because of atrial fibrillation and concomitant coronary artery disease have proven to be safe and effective to prevent embolic events [7]. Only a few reports exist about the combination of antiplatelet and direct oral anticoagulants in left ventricular thrombus patients [8]. Recently published, a multicenter cohort study using DOACs was associated with a greater risk of stroke or systemic embolism compared to warfarin. The DOACs used were dabigatran, rivaroxaban and apixaban [9].
To our knowledge our case is the first describing the newest DOAC edoxaban in this setting, therefore no conclusion for the use of different DOACs can be drawn.
Although randomized studies on duration and composition of anticaogulative medication are lacking, this case may show that complete resolution of LV thrombus with a shorter and less aggressive medical therapy with the newest DOAC agent is possible, especially in a spontaneously recanalized coronary vessel without the need for percutaneous interventional therapy. We postulate that left ventricular thrombi in patients after acute coronary syndromes have to be differently evaluated in comparison to patients without coronary artery disease.
Learning objective / Methods
In a patient with neurological and cardiac symptoms an acute coronary syndrome complicated by the presence of left ventricular embolic thrombi may be the correct diagnosis. Multidisciplinary non - invasive imaging strategy and subsequent personalized anticoagulative therapy to the individual bleeding risk should be started immediately to avoid further ischemic or embolic events.
We confirm that this specific clinical case related study was reviewed and approved by all clinicians involved in the case and, after allowance to publish from the patient's side, we did not seek specific IRB approval.
Statement of Ethics
The published research complies with the guidelines for human studies and was conducted ethically by the WMA Declaration of Helsinki. The subject has given informed consent to publish the case.
Disclosure Statement
The paper is not under consideration elsewhere. There are no disclosures of any relationship with industry for both authors.
Funding Sources
The research did not receive any funding.
Author Contributions
All authors contributed equally to the design, draft and revision of the manuscript.
References
- Ghadri J-R, Wittstein IS, Prassad A et al. International expert consensus document on Takotsubo syndrome (part I): Clinical characteristics, diagnostic criteria, and pathophysiology. Eur Heart J 2018;39:2032-46.
- Chae MK, Kim EK, Jung KY et al. Triple rule-out computed tomography for risk stratification of patients with acute chest pain. J Cardiovasc Comput Tomogr 2016;10:291-300.
- Groeneveld NS, Guglielmi V, Leeflang MMG et al. CT angiography vs echocardiography for detection of cardiac thrombi in ischemic stroke: a systematic review and meta-analysis. J Neurol 2020 doi: 10.1007/s00415-020-09766-8.
- Leow AST, Sia CH, Tan BYQ et al. A meta summary of case reports of non-vitamin K antagonist oral anticoagulant use in patients with left ventricular thrombus. J Thromb Thrombolysis 2018;46:68-73.
- Lattuca B, Bouziri N, Kerneis M, et al. Antithrombotic therapy for patients with left ventricular mural thrombus. J Am Coll Cardiol 2020;75:1676-85.
- Maniwa N, Fujino M, Nakai M et al. Anticoagulation combined with antiplatelet therapy in patients with left ventricular thrombus after first acute myocardial infarction. Eur Heart J 2017; 39:201-8.
- Lip GYH, Collet J-P, Haude M, et al. Management of antithrombotic therapy in AF patients presenting with ACS and/or undergoing PCI. Eur Heart J 2018;39 (31):2847-50.
- Bastiany A, Grenier ME, Matteau A, et al. Prevention of left ventricular thrombus formation and systemic embolism after anterior myocardial infarction: a systematic literature review. Can J Cardiol 2017;33:1229-36.
- Robinson AA, Tranke CR, Eubanks G, et al. Off-label use of direct oral anticoagulants compared with warfarin for left ventricular thrombi. JAMA Cardiology 2020.