-
Address:
17888 67th Court North
Loxahatchee, FL
-
Mail us:
contact@wrightacademia.org
- submit manuscript
Case Report |
Open Access |
Volume 2 | Issue 1 |
Focal Subacute Thyroiditis in a Post-Covid-19 Patient: A Case Report
Anand Hinduja1 and Sanjay Mishra2
1Aarti Clinic, Kharghar, Navi Mumbai, India
2Avneesh Diagnostics, Kharghar, Navi Mumbai, India
*Corresponding author: A Hinduja, Aarti Clinic, 10, Monarch Fortune CHS, Sector 18, Kharghar, Navi Mumbai - 410210, India, Tel: +91-773-813-9997, Email: dranand01@gmail.com
Citation: Hinduja A, Mishra S (2021) Focal Subacute Thyroiditis in a Post-Covid-19 Patient: A Case Report. J SARS-CoV-2 COVID 2:005.
Copyright © Hinduja A, et al.
Received: |
Accepted: |
Published: |
Subacute thyroiditis is an acute inflammatory disorder of the thyroid most commonly due to a viral infection. We hereby describe the case of an apparently healthy 36-year-old female presenting with subacute thyroiditis few weeks after a very mild presentation of COVID-19. The case highlights the utility of C- reactive Protein, Ultrasonography and Color Doppler in arriving at a diagnosis. Prednisolone remains the mainstay of management and is associated with early remission. A high degree of suspicion is required by the treating physician in such patients as the clinical presentation mimics pharyngitis.
Introduction
Subacute thyroiditis is an acute inflammatory disorder of the thyroid most commonly caused due to a viral infection, characterized by fever and tender thyroid, generally associated with a transient episode of hyperthyroidism. We describe a case of an apparently healthy 36-year-old female presenting with subacute thyroiditis few weeks after mild COVID-19 infection. The case highlights the importance of screening for thyroid function in patients presenting with neck pain and fever few weeks after suffering from COVID-19 infection.
Case Report
A previously healthy 36-year-old female presented to the outpatient department with fever and pain in the throat extending to the right ear for a week. The fever was high grade and intermittent with a maximum temperature of 39.4 °C. This was accompanied by unexplained weight loss of 4 kgs in one week. Her medical history was significant for mildly symptomatic COVID-19 infection three weeks back, which was managed at home with antipyretics and vitamin supplements. Her recovery from the infection was uneventful and she tested negative for COVID-19 RT-PCR at the end of her 14-day isolation period. Family history was negative for any chronic disease including Diabetes, Hypertension, Thyroid Disease and Malignancy or any autoimmune disease including Systemic Lupus Erythromatosus (SLE).
On clinical examination, the patient was febrile 38.3 °C with a pulse rate of 116 beats/min, respiratory rate of 16/min, oxygen saturation of 98% on room air, and blood pressure of 110/60 mm of Hg. On palpation of the neck, anterior neck tenderness on the right side was appreciated.
Lab workup revealed elevated C-reactive protein (CRP) at 150 mg/l, Free thyroxine (fT4) and Free triiodothyronine (fT3) levels were elevated at 3.36 ng/dL (ref range 0.89-1.76) and 5.40 pg/ml (ref range 2.3-4.2), respectively. Thyroid-stimulating hormone (TSH) was low at 0.006 micro IU/ml. Thyroid peroxidase antibody and anti-thyroglobulin antibody were negative. Her D dimer levels were < 25 ng/ml FEU, COVID-19 RT PCR was negative, and the COVID-19 total antibody was positive. Complete blood count showed neutrophilic leucocytosis with TLC of 13,900/cumm but infectious disease panel and metabolic profile were normal. Her electrocardiography revealed sinus tachycardia.
Ultrasound of the neck revealed an ill-defined heterogeneously hypoechoic nodule in right lobe of thyroid, at its mid and lower polar level extending up to right half of isthmus (Figure 1). Color Doppler mapping showed moderately increased vascularity, with a diffuse hypervascularization pattern similar to Graves' disease. Increased Peak systolic velocities were noted in right Inferior Thyroid artery (25 to 35 cm/sec) (Figure 2). Few hypoechoic reactive right cervical lymph nodes were seen at levels III, IV & VI.
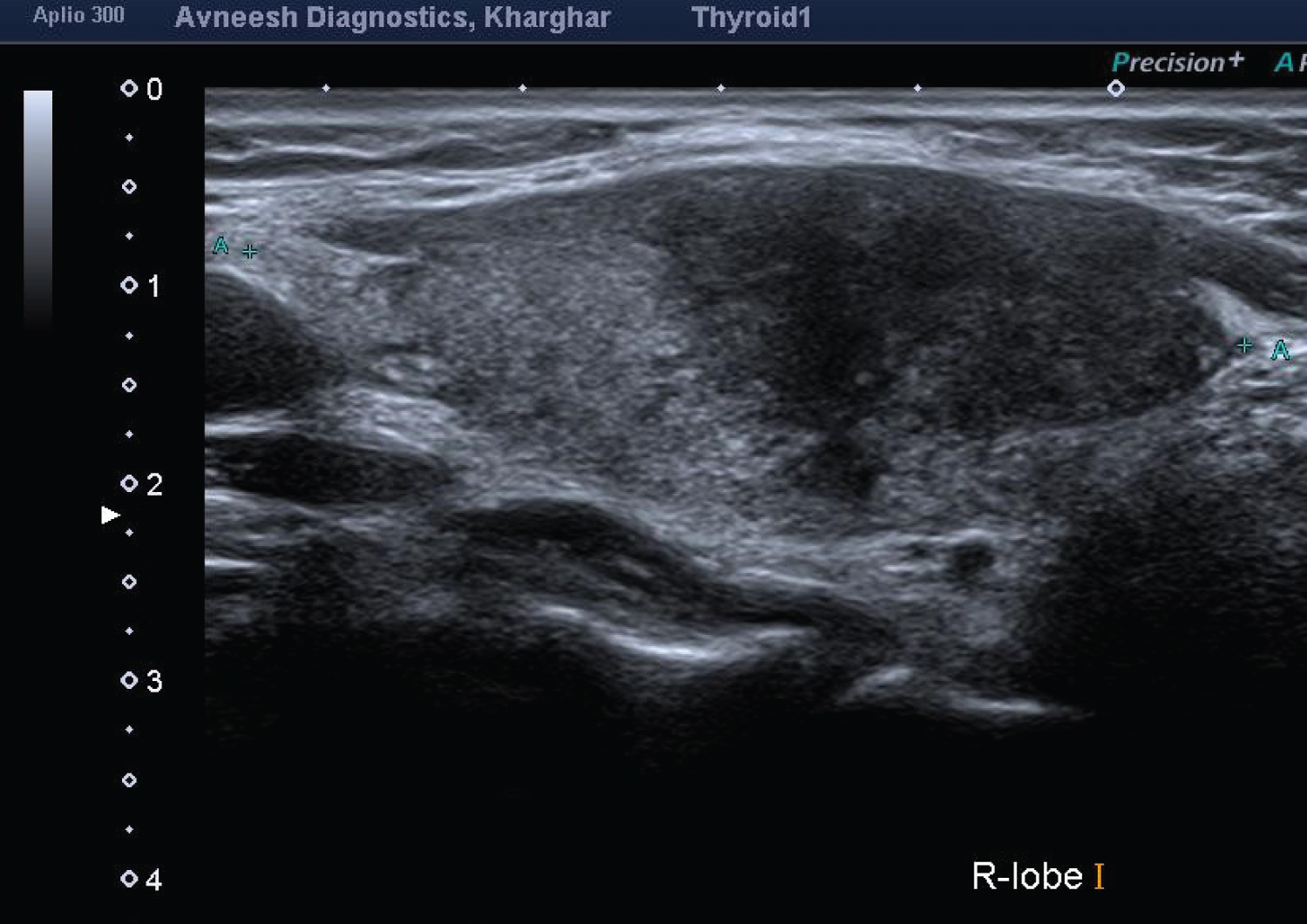
Figure 1: Thyroid ultrasound scanning B-mode.
Thyroid ultrasonography longitudinal scan reveals an inhomogeneous hypoechoic nodule, with irregular poorly defined margins in the right thyroid lobe.
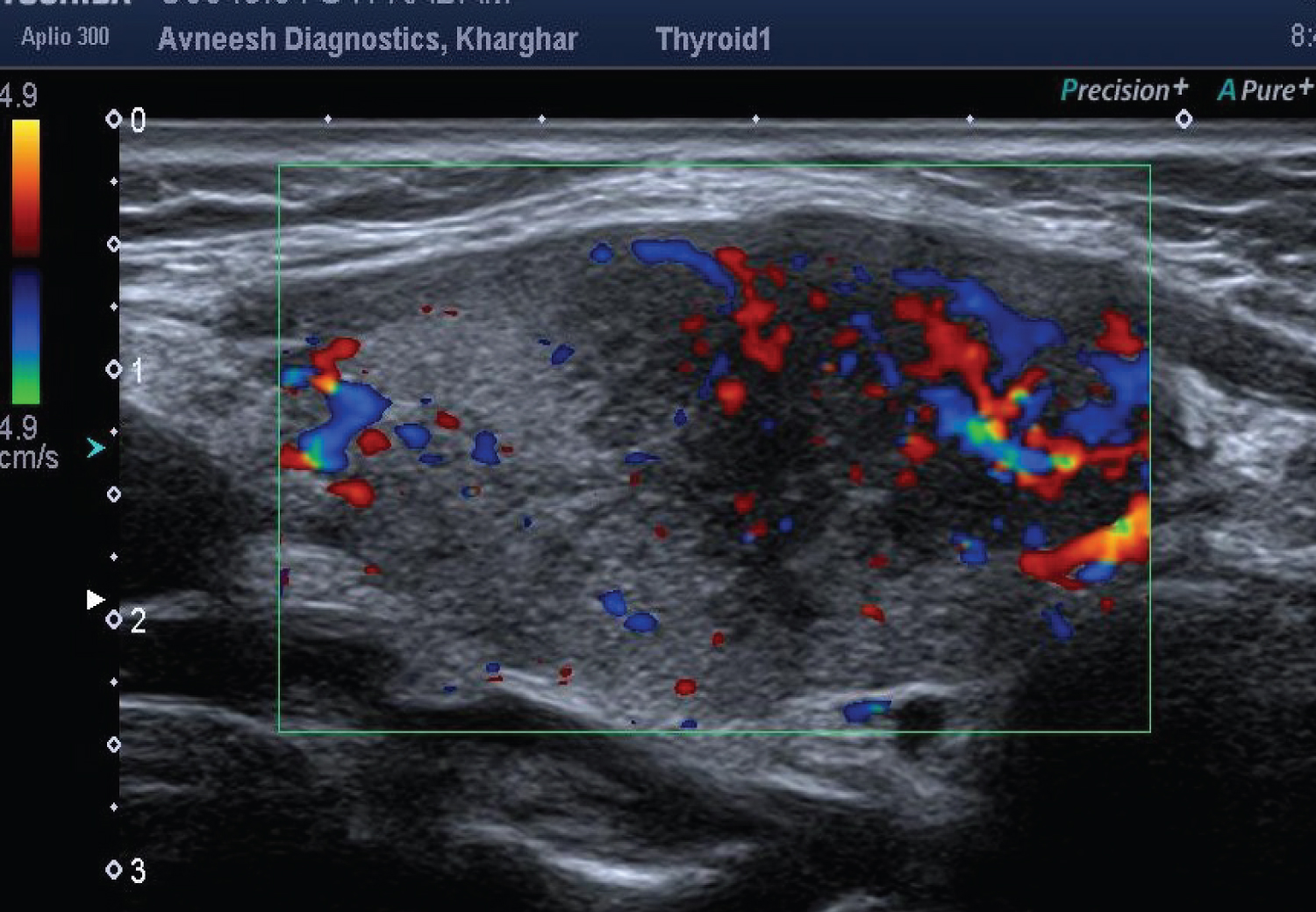
Figure 2: Color doppler of thyroid gland.
Color doppler reveals increased vascularity with in the hypoechoic nodule with hyper vascularization pattern.
A clinical diagnosis of focal subacute thyroiditis was made, and the patient was put on oral prednisolone (20 mg) and Propranolol (40 mg) daily for two weeks. The patient became afebrile within 72 hours but other symptoms persisted. The patient showed continued improvement and was completely asymptomatic after two weeks. The prednisone was gradually tapered off over four weeks, and propranolol was discontinued. The patient remained asymptomatic at eight weeks follow up, and the CRP and thyroid function tests returned to normal. Follow-up ultrasound screening revealed disappearance of the hypoechoic nodule.
Discussion
Subacute thyroiditis is a self-limiting thyroid disorder associated with a triphasic clinical course of hyperthyroidism, hypothyroidism, and return to normal thyroid function. The thyroid gland and viral infections are known to be engaged in complex interplay via hormones and immunomodulatory signalling molecules [1]. In case of SARS-CoV-2, the virus causing coronavirus disease 2019 (COVID-19), two probable mechanisms might account for the changes in the thyroid gland and its hypothalamic-pituitary axis. One is an indirect effect through abnormal systemic inflammatory-immune responses caused by SARS-CoV-2 infection, and another is a direct viral effect [2,3]. Molecular mimicry could also explain the way the virus activates an antiviral response which turns against autoantigens leading to subacute thyroiditis after clinical recovery. SARS-CoV-2 uses the angiotensin-converting enzyme 2 (ACE2) as a cell receptor to invade human cells [4]. The involvement of thyroid in the COVID-19 infection could be attributed to the ACE2 expression levels which were found to be high in the small intestine, testis, kidneys, heart, gall bladder and thyroid [5].
The clinical features in our case were similar to the presentation of subacute thyroiditis. The elevated CRP in this case correlates well with the presentation of Subacute thyroiditis. There is significantly higher rise in serum CRP level in patients with Subacute thyroiditis as compared to patients with Graves' disease [6].
Ultrasound findings in acute phase present as nodular focal form, show irregular and ill-defined hypoechogenic areas/nodule, predominantly in the subcapsular region. Hyperthyroidism symptoms are frequent in this acute phase, attributable to follicular rupture. Hypoechoic nodule, with ill-defined borders, makes it tedious to differentiate from malignant thyroid nodule and can even in some cases require fine needle aspiration biopsy for confirmation [7].
In early stages doppler ultrasound usually shows diffuse hypervascularization, which can be similar to the “thyroid inferno” described in Graves' disease, albeit in a less intense form and with lower systolic velocity peak in the thyroid arteries [8].
There is no definitive treatment of painful subacute thyroiditis. Prednisolone is the preferred glucocorticoid in management of subacute thyroiditis. However, there have been no studies regarding the optimal dose of prednisolone for treatment of subacute thyroiditis. Few studies have been undertaken with low dose of prednisolone over prolonged time to minimize the side effects of high dose steroids [9,10]. We followed a low dose regime of 20 mg/day oral prednisolone and tapered it over four weeks leading to excellent clinical improvement with minimal side-effects.
Most patients of COVID-19 infection are asymptomatic or mildly symptomatic. The case stresses the need to suspect thyroiditis in such patients where the clinical picture mimics pharyngitis. Ultrasonography, thyroid function tests and CRP play a crucial role in diagnosis. Low dose prednisolone is the mainstay of management along with propranolol for symptom relief.
Footnote
Reporting checklist
The authors have completed the CARE reporting checklist.
Conflict of interest
The authors report no conflict of interest.
Ethical statement
This report was in accordance with the Helsinki Declaration. This case report has non-identifiable clinical data of our patient.
References
- Tomer Y, Davies TF (1993) Infection, thyroid disease, and autoimmunity. Endocrine Reviews 14: 107-120.
- Lorenzo S, Pitoia F (2020) Impact of COVID-19 on the thyroid gland: an update. Reviews in Endocrine & Metabolic Disorders 1-13.
- Lania A, Sandri MT, Cellini M, et al. (2020) Thyrotoxicosis in patients with COVID-19: The THYRCOV study. European Journal of Endocrinology 183: 381-387.
- Li W, Moore MJ, Vasilieva N, et al. (2003) Angiotensin-converting enzyme 2 is a functional receptor for the SARS coronavirus. Nature 426: 450-454.
- Hikmet F, Méar L, Edvinsson Å, et al. (2020) The protein expression profile of ACE2 in human tissues. Mol Syst Biol 16: e9610.
- Baruah, Manash P, Bhattacharya B (2012) Significant role of serum CRP in differentiating inflammatory from non-inflammatory causes of thyrotoxicosis. Indian journal of endocrinology andmetabolism 16: 976-981.
- Takahashi MS, Pedro HM, Moraes and Chammas MC (2019) Ultrasound Evaluation of Thyroiditis: A Review. Journal of Otolaryngology Research 2: 127.
- Donkol RH, Nada AM, Boughattas S (2013) Role of color Doppler in differentiation of Graves' disease and thyroiditis in thyrotoxicosis. World Journal of Radiology 5: 178-183.
- Nishihara E, Ohye H, Amino N, et al. (2008) Clinical characteristics of 852 patients with subacute thyroiditis before treatment. Internal Medicine 47: 725-729.
- Koirala Prasad K, Sharma V (2015) Treatment of Acute Painful Thyroiditis with Low Dose Prednisolone: A Study on Patients from Western Nepal. Journal of Clinical and Diagnostic Research 9: MC01-MC03.