-
Address:
17888 67th Court North
Loxahatchee, FL
-
Mail us:
contact@wrightacademia.org
- submit manuscript
Review Article |
Open Access |
Volume 1 | Issue 1 |
Who Should Get Extended Thromboprophylaxis after Hip Fracture Surgery? A Database Study Examining Risk Factors for Post Discharge Venous Thromboembolism
Aria Darius Darbandi1, Ghulam H Saadat2, Bennet A Butler3, Faran Bokhari2 and Ghulam H Saadat, MD2*
1California University of Science and Medicine, Colton, USA
2Department of Trauma and Burn Surgery, John H Stroger Hospital of Cook County, Chicago, USA
3Department of Orthopedic Surgery, Northwestern Memorial Hospital, Chicago, IL, USA
*Corresponding author: Ghulam H Saadat, MD, Department of Trauma and Burn Surgery, John H Stroger Hospital of Cook County, 1950 W Polk St, Chicago, IL 60612, USA, Tel: 0017404478675, Fax: 003128649169, E-mail: ghulam.saadat@cookcountyhhs.org
Citation: Darbandi AD, Saadat GH, Butler BA, Bokhari F, Saadat GH (2021) Who Should Get Extended Thromboprophylaxis after Hip Fracture Surgery? A Database Study Examining Risk Factors for Post Discharge Venous Thromboembolism. J Surg Clin Rpts 1:010.
Copyright © Darbandi AD, et al.
Received: |
Accepted: |
Published: |
Objective
The purpose of this study was to evaluate factors associated with post-discharge venous thromboembolism (VTE) within 30-days of hip fracture surgery.
Method
96,870 cases with acute hip fractures were identified from a national retrospective database. We only included patients who received intramedullary nail fixation, extramedullary implant fixation, or hemiarthroplasty.
Results
Factors associated with post-discharge VTE include age above 75, 5-item modified frailty index ≥ 0.6, COPD, dyspnea, disseminated cancer, chronic steroid use, intramedullary nailing, medical co-management, and pathological fractures.
Conclusions
The current study suggests specific factors independently associated with post-discharge VTE following hip fracture.
Introduction
Postoperative venous thromboembolism (VTE) is a common and potentially lethal complication of hip fracture surgery [1,2]. The implementation of proper prophylactic measures such as the administration of anticoagulation agents, frequent ambulation, and the use of intermittent pneumatic compression devices have significantly reduced the rate of postoperative VTE [1]. While institutions may differ in their specific protocol, anticoagulation therapy remains the cornerstone of postoperative VTE prophylaxis, as these agents are highly effective if properly administered [2]. However, the duration of VTE prophylaxis is still a matter of debate.
Extending anticoagulation beyond the standard duration of 6-14 days following surgery is an effective way to limit post-discharge VTE occurrence in high-risk patients [3,4]. However, not all patients are suitable to receive extended anticoagulation, as the risk of hemorrhage may outweigh the benefits of prophylaxis [4,5]. Therefore, it is crucial that surgeons can identify those who may require additional anticoagulation therapy. Certain preoperative characteristics such as higher BMI, older age, smoking, and cancer have been identified as risk factors postoperative VTE [2,6-9]. Postoperative factors such as extended operational time and immobility may also increase the risk of VTE [1]. Currently, there has not been a large-scale, nationwide analysis examining the risk factors of VTE among hip fracture patients following hospital discharge to guide surgeons whether extended anticoagulation prophylaxis is appropriate.
The aim of this investigation was to evaluate variables associated with post-discharge VTE within 30-days of hip fracture surgery. The large-scale nature of this investigation will allow us to identify overlooked factors that may leave patients susceptible to VTE following discharge. The goal of this analysis is to help surgeons determine who should receive extended anticoagulation therapy following hip surgery.
Material and Methods
Study population
This study was conducted utilizing patient data from the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP). ACS-NSQIP is a validated database that prospectively collects detailed information from patients undergoing major surgical procedures from over 600 participating hospitals across the United States [10]. Hip fracture cases were identified using International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10 CM) codes for "fracture of head or neck of femur" (S72.0) and "pertrochanteric fracture" (S72.1). Only initial encounter cases were included in the study. Current Procedural Terminology (CPT) codes were utilized to identify patients who underwent open reduction internal fixation (CPT = 27245 and CPT = 27244) or hemiarthroplasty (CPT = 27236) of hip fractures between January 1, 2016, to December 31, 2019. As our primary study variable was post-discharge VTE, patients who developed VTE within their hospital stay were excluded from the analysis.
Post-discharge venous thromboembolism
This study's primary outcome variable was post-discharge VTE, defined as either the occurrence of deep vein thrombosis (DVT) or pulmonary embolism (PE) after a patient was discharged from the hospital and within 30-days of hip fracture surgery. ACS-NSQIP defines DVT as a new venous thrombosis confirmed by imaging and requiring therapy. Only PE cases confirmed by modalities such as CT scan pulmonary angiogram, ventilation-perfusion lung scan, or direct autopsy were included in the ACS-NSQIP dataset.
Study variables
This study's demographic and lifestyle variables were age, gender, body mass index (BMI), functional status, and smoking. Comorbidities examined in this study were hypertension (HTN), diabetes mellitus (DM), congestive heart failure (CHF), chronic obstructive pulmonary disease (COPD), dyspnea on exertion, anemia, disseminated cancer, preoperative dialysis, steroid use, bleeding disorders, and > 10% body weight loss in the last 6 months. Patients with a preoperative hematocrit of < 41% for males and < 36% for females were considered anemic. American Society of Anesthesiologists (ASA) classification and the 5-item modified frailty index (5i-mFI) were assessed in this study. ASA classifications were grouped as either low risk (class I and II), medium risk (class III), or high risk (class IV and V). The 5i-mFI has been used as a predictive index for postoperative complications following orthopedics surgery. 5i-mFI is calculated using the presence of five comorbidities: CHF, HTN, DM (either insulin-dependent or noninsulin-dependent), COPD, and functional dependent status (either partially or completely dependent).
Procedural and medical factors examined in this study were operation duration, pre-operative and post-operative length of stay (LOS), surgical technique, elective cases, fracture type, medical co-management, hip fracture care program, pathological fracture, post-operative weight bearing status, and the extension of thromboprophylaxis to at least 28 days postoperatively. Definitions for each variable can be found in the ACS-NSQIP user guide [10].
Statistical analysis
All analyses were conducted using SPSS Statistics 27.0.1 (IBM Corporation, Armonk, NY). Pre-operative and post-operative LOS were defined as continuous, non-parametric variables and described using mean ± standard deviation. All other variables were categorical and expressed as frequency and percentage. Procedural duration was stratified as either longer or shorter than 1 hour. Descriptive analysis was carried out and stratified based on the occurrence of post-discharge VTE. Bivariate analyses were carried out using chi-square and two-sided Fisher's exact tests for categorical variables. Mann-Whitney U test was used for nonparametric continuous variables. Multivariable analysis for the binary outcome of post-discharge VTE was conducted using multiple logistic regression models adjusted for age, gender, smoking status, BMI, 5m-FI, functional status, and history of bleeding disorders. Multivariable analysis for preoperative LOS was conducted using a linear regression model adjusting for the same variables as the logistic regression models. Cases with missing information were excluded on a list-wise basis for both bivariate and multivariate analyses. For all analyses, the level of statistical significance was set as α = 0.05 (2-tailed).
Results
In the current study, 96,870 hip fracture cases that underwent surgery were included. The frequency of post-discharge VTE was 0.9% (n = 880). The 30-day distribution of postoperative DVT and PE is outlined in Figure 1. The preoperative characteristics of our study population are outlined in Table 1. Most patients were above the age of 75 (62.0%, n = 47,052/75,940), female (69.1%, n = 66,968), had normal weight (46.5%, n = 42,043/90,503), and a 5i-mFI score of 0.2 (43.3%, n = 41,546/96,047). Compared to those without post-discharge VTE, patients with post-discharge VTE were more often older than 75 years (65.9% vs. 61.9%, p = 0.034), obese (15.6% vs. 20%, p < 0.001), 5i-mFI ≥ 0.6 (7.5% vs. 9.4%, p = 0.015), and functionally independent (81.3% vs. 78.2%, p = 0.030). Also, patients who developed post-discharge VTE had higher rate of disseminated cancer (6.5% vs. 2.9%, p < 0.001), dyspnea (9.9% vs. 7.7%, p = 0.02), or were on chronic steroid therapy (7.7% vs. 5.3%, p = 0.002).
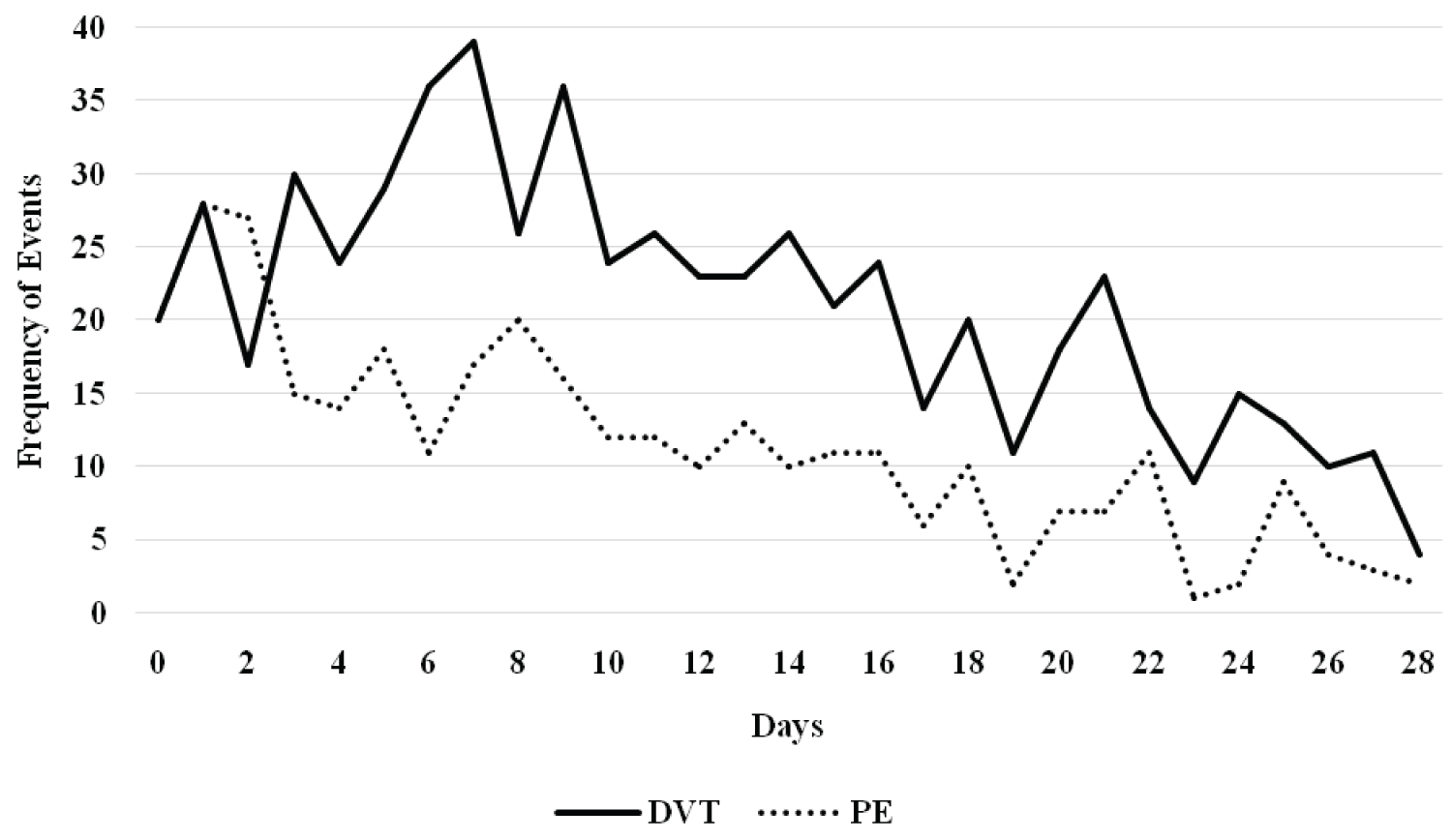
Figure 1: Occurrence of post-discharge deep veinous Thrombosis and pulmonary embolism.
Operative and postoperative characteristics of the study are presented in Table 2. Overall, majority of fractures were pertrochanteric (57.4%, 40,877) and were treated with intramedullary nailing (53.0%, 51,298). 61.7% (27,531/44,640) of patients received extended DVT prophylaxis, and 0.9% (880) of patients developed VTE following hospital discharge. The morality rate was 5.4% (5,252) and readmission rate was 10.2% (8,005/78,118). Patients who developed VTE suffered more often from pertrochanteric fractures (62.3% vs. 57.3%, p = 0.012), underwent intramedullary nailing (p < 0.001), and had procedures longer than 1 hour (49.2% vs. 45.4%, p = 0.027). Patients with post-discharge VTE were more often medically co-managed (93.6% vs. 88.4%, p < 0.001) or suffered from pathological fractures (6.9% vs. 4.6%, p = 0.048). Post-discharge VTE patients had lower rates of enrollment in hip fracture care programs (50.6% vs. 58.3%, p = 0.002). Patients with post-discharge VTE had higher rates of CVA (1.7% vs. 0.2%, p < 0.001), MI (4.5% vs. 0.5%, p < 0.001), readmission (59.9% vs. 9.7%, p < 0.001), and mortality (7.3% vs. 5.4%, p < 0.001).
Table 2: Patients' operative variables and postoperative outcomes. View Table 2
Results of the multivariable analysis are outlined in Table 3. Risk factors significantly associated with VTE were age above 75 years (OR 1.249, CI 1.052-1.483, p = 0.011), BMI ≥ 30 (OR 1.491, CI 1.211-1.835, p < 0.001), 5i-mFI ≥ 0.6 (OR 1.38, CI 1.039-1.831, p = 0.026), history of COPD (OR 1.379, CI 1.058-1.798, p = 0.018), dyspnea (OR 1.342, CI 1.036-1.739, p = 0.026), disseminated cancer (OR 2.573, CI 1.935-3.422, p < 0.001), chronic steroid use (OR 1.447, CI 1.099-1.904, p = 0.008), IMN (OR 1.344, CI 1.022-1.766, p = 0.034), medical co-management (OR 1.613, CI 1.029-2.528, p = 0.037), and pathological fractures (OR 1.54, CI 1.015-2.336, p = 0.043). Variables associated with lower rate of post-discharge VTE were enrollment in a hip fracture care program (OR 0.77, CI 0.614-0.965, p = 0.024), preoperative dialysis (OR 0.457, CI 0.216-0.967, p = 0.04), and anemia (OR 0.841, CI 0.714-0.991, p = 0.038). Patients who developed post-discharge VTE were associated with higher odds of stroke (OR 8.62, CI 4.739-15.625, p < 0.001), MI (OR 10.638, CI 7.3-15.625, p < 0.001), readmissions (OR 16.393, CI 13.333-20, p < 0.001), and mortality (OR 1.748, CI 1.28-2.387, p < 0.001).
Table 3: Multivariable analysis for the association of post-discharge VTE. View Table 3
Discussion
VTE is a common and potentially preventable postoperative complication of hip fracture surgery [1,2]. This study found that 0.9% of patients undergoing hip fracture surgery developed VTE following discharge. This was significantly lower compared to 14% postoperative VTE rates previously reported in orthopedic trauma patients [1,11]. Our investigation, in agreement with previous literature, showed that the patients who develop post-discharge VTE were associated with worse clinical outcomes, including MI, CVA, readmission, and mortality [1]. Extending anticoagulation therapy can limit postoperative VTE rate and lead to better clinical outcomes among high-risk patients undergoing major orthopaedic procedures [3,4]. While the prophylactic benefit of anticoagulation has been previously studied, this study aims to identify patients who are at high-risk of post-discharge venous thromboembolism and may benefit from extended thromboprophylaxis. This information is essential for surgeons, as there is currently a lack of large-scale, nationwide data examining the risks associated with post-discharge VTE.
Various preoperative characteristics were identified in our multivariable analysis to be associated with post-discha fax rge VTE. Our study found an elevated adjusted risk for post-discharge VTE in patients above the age of 75. In addition to increased rates of immobility, comorbidities, and worse clinical outcomes, elderly patients are more likely to develop postoperative VTE, possibly secondary to vascular sclerosis and higher blood viscosity [2,6,12,13]. This investigation also found that patients with a BMI greater than 30 had an elevated adjusted risk of post-discharge VTE compared to patients with BMIs within the normal range (18.5-24.9). Elevated BMI has often been cited as a risk factor for postoperative VTE, leading many to advocate more aggressive anticoagulation therapy in obese patients [11]. COPD, chronic steroid use, pathological fractures, and disseminated cancer are known factors for VTE [8,9,11]. In the current study, the aforementioned factors were also associated with post-discharge VTE. Comorbidities such as CHF, DM, HTN, and COPD individually failed to reach significance with post-discharge VTE; however, a significant association was found when comorbidities were factored in the 5i-mFI. This suggests that patients who have multiple comorbidities may benefit from extended thromboprophylaxis [2,14,15].
Our investigation identified IMN as a risk factor for post-discharge VTE, an association scarcely described prior to this study [8,9,16]. In a prospective, single-institution study of 5,300 hip fracture cases, McNamara, et al. found that patients undergoing IMN had significantly higher rates of VTE (3.3%) compared to patients undergoing sliding hip screw (2.9%) and hemiarthroplasty (1.7%) [16]. Higher VTE risk may be due to increased intramedullary canal pressure during IMN, which can disrupt the venous blood system and manifest into post-operative emboli [17]. Awareness of this association may aid in management.
Medical co-management was found to be associated with an elevated risk of post-discharge VTE. While co-management between orthopaedic surgeons and geriatricians is an evolving practice that may offer benefits in healthcare costs, the current literature is conflicting on whether these patients truly benefit from better clinical outcomes [18,19]. Disruptions in the continuity of care of these patients may lead to higher rates of postoperative complications, including VTE. However, it is important to note these patients tend to be more ill and suffer from higher acuity injuries [18]. Nevertheless, our study suggests that co-managed patients should be monitored closely for post-discharge VTE. Conversely, our study found that patients enrolled in hip fracture care programs were less likely to develop post-discharge VTE. Comprehensive care programs have been associated with better clinical outcomes and reduced mortality among hip fracture patients, especially in those above the age of 60 [20,21]. These care programs may be advantageous to those at high risk of post-discharge VTE.
Our study has a series of limitations to consider. This analysis was retrospective, making it susceptible to coding flaws and residual cofounding bias. The primary outcome of VTE only includes cases that were confirmed by testing, potentially excluded several unrecognized events. However, one investigation found that the reported rate of surveillance detected DVT following high-risk procedures in ACS NSQIP is comparable to symptomatic DVT rates [22]. Furthermore, this study was limited by unavailable information detailing the level of thromboprophylaxis each patient received, potentially affecting our results. For instance, this study identified preoperative dialysis and anemia, known factors to contribute to thromboembolism, as protective factors for VTE [23,24]. Furthermore, risk factors that were expected to lead to VTE such as smoking and shortened duration of thromboprophylaxis failed to make the appropriate associations [3,4,7]. While some of these discrepancies are in line with findings from other large-database studies, these observations were more than likely due to variations inpatients' clinical management, as high-risk patients will generally raise concern for postoperative VTE and receive additional prophylaxis measures. This study would have benefited if the ACS NSQIP dataset provided information such as the use of compression devices, inferior vena cava filter placements, and the specific agents used for thromboprophylaxis [11].
Conclusions
This study is the first to examine the risk factors for VTE following hospital discharge in hip fracture patients. In addition to confirming well-known risk factors for VTE such as age and obesity, our study found that IMN, medical co-management, and high 5i-mFI score were associated with post-discharge VTE. Our study results also indicated that patient factors including age ≥ 75 years, obesity, steroid use, disseminated cancer, and pathological fractures may warrant extended anticoagulation following hip fracture. Patients who were treated with IMN or were medically co-managed may benefit from extended anticoagulation as well. Lastly, hip fracture care programs can help limit the occurrence of post-discharge VTE and should be encouraged in high-risk patients.
Disclosure of Interest
None.
Author Contributions
Conception and design: Saadat and Darbandi; Acquisition of data: Saadat; Statistical analysis of data: Darbandi Interpretation of data: All authors; Drafting of the manuscript: Darbandi and Saadat; Critical revision of the manuscript for important intellectual content: Butler and Bokhari; Final revision of the version to be published: All authors; Administrative, technical, or material support: Bokhari; Supervision: Bokhari.
References
- Schiff RL, Kahn SR, Shrier I, et al. (2005) Identifying orthopaedic patients at high risk for venous thromboembolism despite thromboprophylaxis. Chest 128: 3364-3371.
- White RH (2003) The epidemiology of venous thromboembolism. Circulation 107: I4-8.
- Huo MH, Muntz J (2009) Extended thromboprophylaxis with low-molecular-weight heparins after hospital discharge in high-risk surgical and medical patients: A review. Clin Ther 31: 1129-1141.
- Hull RD, Pineo GF, Stein PD, et al. (2001) Extended out-of-hospital low-molecular-weight heparin prophylaxis against deep venous thrombosis in patients after elective hip arthroplasty: A systematic review. Ann Intern Med 135: 858-869.
- Lee R, Lee D, Gowda NB, et al. (2019) Surgical complications associated with congestive heart failure in elderly patients following primary hip hemiarthroplasty for femoral neck fractures. Eur J Orthop Surg Traumatol 29: 1253-1261.
- White RH, Zhou H, Gage BF (2004) Effect of age on the incidence of venous thromboembolism after major surgery. J Thromb Haemost 2: 1327-1333.
- Platzer P, Thalhammer G, Jaindl M, et al. (2006) Thromboembolic complications after spinal surgery in trauma patients. Acta Orthop 77: 755-760.
- Shallop B, Starks A, Greenbaum S, et al. (2015) Thromboembolism After Intramedullary Nailing for Metastatic Bone Lesions. J Bone Joint Surg Am 97: 1503-1511.
- Piccioli A, Rossi B, Scaramuzzo L, et al. (2014) Intramedullary nailing for treatment of pathologic femoral fractures due to metastases. Injury 45: 412-417.
- ACS NSQIP 2019 PUF USER GUIDE.
- Whiting PS, White-Dzuro GA, Greenberg SE, et al. (2016) Risk Factors for Deep Venous Thrombosis Following Orthopaedic Trauma Surgery: An Analysis of 56,000 patients. Arch Trauma Res 5: e32915.
- Nam J-H, Kim D-H, Yoo J-H, et al. (2017) Does preoperative mechanical prophylaxis have additional effectiveness in preventing postoperative venous thromboembolism in elderly patients with hip fracture?-Retrospective case-control study. PLoS One 12: e0187337.
- Kang J, Jiang X, Wu B (2015) Analysis of Risk Factors for Lower-limb Deep Venous Thrombosis in Old Patients after Knee Arthroplasty. Chin Med J (Engl) 128: 1358-1362.
- Wang S, Zhao Y (2013) Diabetes mellitus and the incidence of deep vein thrombosis after total knee arthroplasty: A retrospective study. J Arthroplasty 28: 595-597.
- Kapoor A, Labonte AJ, Winter MR, et al. (2010) Risk of venous thromboembolism after total hip and knee replacement in older adults with comorbidity and co-occurring comorbidities in the Nationwide Inpatient Sample (2003-2006). BMC Geriatr 10: 63.
- McNamara I, Sharma A, Prevost T, et al. (2009) Symptomatic venous thromboembolism following a hip fracture. Acta Orthop 80: 687-692.
- Giannoudis PV, Tzioupis C, Pape H-C (2006) Fat embolism: the reaming controversy. Injury 37: S50-S58.
- Patel NK, Ko CY, Meng X, et al. (2020) Does Comanagement of Patients With Hip Fracture Influence 30-Day Outcomes. Geriatr Orthop Surg Rehabil 11.
- Fisher AA, Davis MW, Rubenach SE, et al. (2006) Outcomes for older patients with hip fractures: the impact of orthopedic and geriatric medicine cocare. J Orthop Trauma 20: 172-178; discussion 179-180.
- Pedersen SJ, Borgbjerg FM, Schousboe B, et al. (2008) A comprehensive hip fracture program reduces complication rates and mortality. J Am Geriatr Soc 56: 1831-1838.
- Kates SL (2016) Hip fracture programs: Are they effective? Injury 47: S25-S27.
- De Martino RR, Beck AW, Edwards MS, et al. (2012) Impact of screening versus symptomatic measurement of deep vein thrombosis in a national quality improvement registry. J Vasc Surg 56: 1045-1051.
- Molnar AO, Bota SE, McArthur E, et al. (2018) Risk and complications of venous thromboembolism in dialysis patients. Nephrol Dial Transplant 3: 874-880.
- Feng L, Xu L, Yuan W, et al. (2020) Preoperative anemia and total hospitalization time are the independent factors of preoperative deep venous thromboembolism in Chinese elderly undergoing hip surgery. BMC Anesthesiol 20: 72.
Table 1: Patients' demographics and clinical characteristics. View Table 1