-
Address:
17888 67th Court North
Loxahatchee, FL
-
Mail us:
contact@wrightacademia.org
- submit manuscript
Research Article |
Open Access |
Volume 1 | Issue 1 |
Utilize an Impella Port and Vascular Graft to the Axillary Artery for TAVR with Poor Femoral Access
Firas Ajam1, Koroush Asgarian2, Brook Dejene2, Matthew D Saybolt3, Dawn Calderon DO4, Brett Sealove4, Richard M Neibart2 and Michael P Carson1
1Division of General Internal Medicine, Seton Hall Hackensack-Meridian School of Medicine, Jersey Shore University Medical Center, USA
2Division of Thoracic Surgery, Seton Hall Hackensack-Meridian School of Medicine, Jersey Shore University Medical Center, USA
3Division of Cardiology, Jersey Shore University Medical Center, USA
4Division of Cardiology, Seton Hall Hackensack-Meridian School of Medicine, Jersey Shore University Medical Center, USA
*Corresponding author: Michael P Carson, MD, Core Associate Professor of Medicine and Obstetrics & Gynecology, Division of General Internal Medicine, Seton Hall Hackensack-Meridian School of Medicine, Jersey Shore University Medical Center. 19 Davis Ave. 6th Floor, Neptune NJ 07753, USA, Tel: 732-776-4826, E-mail: Michael.Carson@hackensackmeridian.org
Citation: Ajam F, Asgarian K, Dejene B, Saybolt MD, Dawn CDO, et al. (2019) Utilize an Impella Port and Vascular Graft to the Axillary Artery for TAVR with Poor Femoral Access. Cardiol Cases Syst Rev. 1:002.
Copyright © Ajam F, et al.
Received: |
Accepted: |
Published: |
Transcatheter aortic valve replacement (TAVR) is approved for patients with severe symptomatic aortic stenosis deemed high risk for open replacement. Subclavian approach is the most common alternative to femoral arterial vessel access in patients with iliofemoral peripheral arterial occlusive disease. We describe a novel technique to obtain trans-axillary access using an end to side vascular graft. This approach minimizes vessel trauma and bleeding, requires a small arteriotomy, offers a short catheter system delivery course with minimal friction, and provides the operator a vascular access site without the physical constraints of a small operative field.
Introduction
Transcatheter aortic valve replacement (TAVR) is approved for patients with severe symptomatic aortic stenosis deemed intermediate, high or prohibitive risk for open replacement [1]. The access site is based upon a pre-determined measurement of arterial luminal diameters, extent of calcification, and degree of tortuosity [2]. National registry data shows that the trans-femoral route is utilized for 65-83% of cases and subclavian artery access is utilized when trans-femoral access is unfavorable or prohibitive [3,4]. Herein, we describe a novel approach to trans-axillary TAVR access in a patient with inadequate femoral vessel size utilizing a vascular graft to introduce the arterial sheath, requiring only a small arteriotomy and potentially minimizing risks including but not limited to vascular complications.
Technique
An 81-year-old male with a past history of paroxysmal atrial fibrillation, chronic obstructive pulmonary disease, and gastrointestinal bleeding due to arterio-venous malformation presented with severe symptomatic normal flow high gradient aortic stenosis (Stage D1, valve area 0.73 cm2). His society of thoracic surgeons predicted risk of operative mortality was 2.6%, risk of morbidity OR mortality was 13.8%, and considered his frailty he was deemed high-risk for surgical replacement and thus was offered TAVR.
Preoperative computerized tomographic angiography revealed the diameter of both external iliac arteries to be < 4mm which are too small, so we proceed with alternative access site. In the operating room general anesthesia was induced without incident. The right axillary artery was identified using intra-operative ultrasound. A horizontal skin incision was made 2 centimeters below the clavicle over the ultrasound marking, dissection was carried down through subcutaneous tissue and pectoral fascia, and a muscle sparing dissection was performed to expose the clavi-pectoral fascia. The axillary artery was isolated with care taken to avoid the neurovascular bundle. Intravenous heparin was given to achieve an activated clotting time of greater than 250. A 10 mm by 15 cm Vascutek Gelweave graft (Terumo Ann Arbor, MI) was beveled and sewn to the axillary artery in an end to side anastomosis (Figure 1). The distal end of the graft was snorkeled outside of the surgical field. The access port of an Impella 5.0 (Abiomed, Danvers, MA) axillary insertion kit closely approximates the size of the TAVR deployment system; the port was placed into the free end of the graft and secured with silk ties (Figure 1). The right femoral artery was accessed using Seldinger technique under ultrasound guidance, and then a 6 French Expo pigtail catheter (Boston Scientific, Natick, MA) was advanced over a 0.035" J wire and placed at the base of the non-coronary cusp of the aortic root. Via the axillary artery graft, we advanced a 6F AL1 catheter over an 0.035" J wire to the aortic root, and then over a 0.035" straight tipped moveable core guidewire, we crossed into the left ventricle in the usual fashion. The AL1 was exchanged for a 6F pigtail catheter (Boston Scientific, Natick, MA) and after a hemodynamic evaluation, the pigtail catheter was exchanged for a 0.035" Medtronic Confida guidwire (Medtronic Inc, Minneapolis, MN). The sheathless Medtronic Evolut R Enveo valve delivery system (Medtronic Inc, Minneapolis, MN) was then inserted into the Impella sheath and advanced without resistance through the Vacate Gel weave graft (Figure 2). Using fluoroscopic guidance, the axillary artery anastomosis was crossed, the delivery system was advanced across the stenotic aortic valve, the TAVR valve was unsheathed and deployed using transesophageal echocardiographic guidance in the usual fashion and the delivery system was then removed. The Gel weave graft was cut 3 mm from the arteriotomy, over sewn, and the incision was then closed in 3 layers.
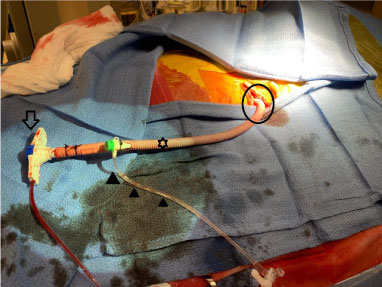
Figure 1: Shows the insertion kit adapted for axillary artery access. Impella 5.0 access device (HOLLOW ARROW) placed into the distal/free end of the Vasotec Gel weave graft (STAR) and secured with silk ties. Distal end of the Gel weave graft (CIRCLE) was anastomosed to the axillary artery in an end-to-side fashion. The 6F × 11 cm sheath (FILLED ARROWHEADS) can be used to advance a 6F Pigtail diagnostic catheter and avoid the need for other arterial access.
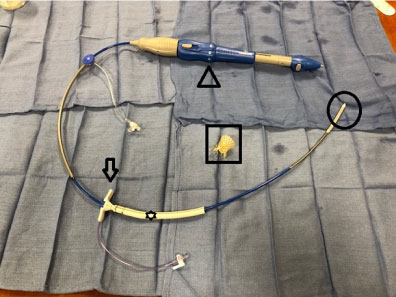
Figure 2: Demonstrates the final setup of the kit adapted for axillary artery access for the Transvalvular Aortic Valve Replacement (TAVR). The TAVR device (ARROWHEAD) was inserted into the external port of the Impella 5.0 insertion kit (ARROW), passed through the Vacate Gel weave graft (STAR), and the distal end of the TAVR device (CIRCLE) was passed through the axillary artery to the aortic valve. The Prosthetic aortic valve is pictured inside the SQUARE.
Comment
Femoral arterial access is the preferred approach to TAVR offering a mortality benefit to alternative access. However, TAVR can be achieved through multiple sites including axillary-subclavian arteries, the left ventricular apex, or the ascending aorta [5]. Axillary-subclavian artery access offers advantages largely related to the shorter distance to the aortic valve including: avoidance of the need to navigate multiple long segments of tortuous arteries, less bowing of the delivery sheath, and better control of the device [5]. The subclavian approach was associated with the need for valve-in-valve implantation to address severe post-TAVR paravalvular leak in only 5.6% of cases compared to 14.8% when the femoral approach was used [7]. Finally, while this number is likely affected by selection bias, a series of 514 patients noted procedural success in 100% of patients utilizing subclavian access vs. 98.4% via the femoral route [7]. In contrast to a report utilizing graft access with a large femoral sheath that must be cut by the operator before being used, the Impella insertion kit seats well within the graft and is the proper length [3]. Additionally, utilizing a vascular graft to introduce the arterial sheath offers the following advantages: low trauma vascular access vessel, minimal blood loss, strong support for the device, preserved ability to perform salvage valvular or coronary interventions if needed, and the shorter course decreases friction on the deployment device allowing greater flexibility and ease of manipulation. The incidence of vascular access complications during TAVR is declining, but still associated with early and late mortality. Preparing for, acknowledging, and addressing these concerns are pivotal to achieving both surgical success and minimize adverse vascular outcomes. When transfermoral access cannot be performed, an axillary-subclavian approach is typically preferred over transapical and direct aortic access as these are deemed "surgical" procedures and increase patient morbidity especially in an older, frail patient cohort.
Additional research and/or registries are necessary to realize how the safety of our approach compares to traditional open subclavian artery cutdowns, other alternative access approaches, or the recently described percutaneous fully percutaneous trans-axillary approach [8].
Acknowledgement
We would like to acknowledge the Jersey Shore University Center Department of Surgery for providing the images for our project.
Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Source
The project was not supported by any grant or funding agencies.
References
- (2017) FDA expands use of Sapien 3 artificial heart valve for high-risk patients.
- Ramlawi B, Anaya-Ayala JE, Reardon MJ (2012) Transcatheter aortic valve replacement (TAVR): access planning and strategies. Methodist Debakey Cardiovasc J 8: 22-25.
- Biasco L, Ferrari E, Pedrazzini G, Faletra F, Moccetti T, et al. (2018) Access Sites for TAVI: Patient Selection Criteria, Technical Aspects, and Outcomes. Front Cardiovasc Med 5: 88.
- Watson DR, Yakubov SJ, Lyons JM, Sanchez Soto CE, Kander NH, et al. (2017) Trans-subclavian approach for transcatheter aortic valve replacement. Ann Cardiothorac Surg 6: 565-567.
- Van Mieghem NM, Tchetche D, Chieffo A, Dumonteil N, Messika-Zeitoun D, et al. (2012) Incidence, predictors, and implications of access site complications with transfemoral transcatheter aortic valve implantation. Am J Cardiol 110: 1361-1367.
- Caceres M, Braud R, Roselli EE (2012) The axillary/subclavian artery access route for transcatheter aortic valve replacement: a systematic review of the literature. Ann Thorac Surg 93: 1013-1018.
- Petronio AS, De Carlo M, Bedogni F, Marzocchi A, Klugmann S, et al. (2010) Safety and efficacy of the subclavian approach for transcatheter aortic valve implantation with the CoreValve revalving system. Circ Cardiovasc Interv 3: 359-366.
- Hallak A, Wei L, Berzingi C, Moreland J, Alkhouli M (2018) Percutaneous axillary access for large-bore arteriotomy: A step-by-step guide. J Card Surg 33: 270-273.